
2025 INDIVIDUAL PLANS
2025 INDIVIDUAL & FAMILY PLANS
Individual and family plans are for people who don’t get insurance through their job and don’t qualify for Medicaid or Medicare. Depending on your income and family size, you may qualify for help paying for your monthly premium.
If you live in Salt Lake or Davis County (* except Bingham Canyon—zip code 84006), you are eligible for U Health Plus — the lowest-premium product offered by University of Utah Health Plans.
Healthy Premier is one of Utah’s largest provider networks with access to U of U Health, Holy Cross Hospitals, MountainStar Healthcare, Ogden Clinic, Granger, Premier, Revere, and many other local, award-winning hospitals and providers.
Highlights
Select a plan for more details
- Healthy Premier Gold COPAY
- U HEALTH PLUS GOLD
- HEALTHY PREMIER GOLD STANDARD
- U HEALTH PLUS GOLD STANDARD
- HEALTHY PREMIER SILVER ELECT COPAY (OFF)
- HEALTHY PREMIER SILVER COPAY
- U HEALTH PLUS SILVER
- HEALTHY PREMIER SILVER STANDARD
- U HEALTH PLUS SILVER STANDARD
- U HEALTH PLUS BRONZE
- HEALTHY PREMIER EXPANDED BRONZE STANDARD
- U HEALTH PLUS EXPANDED BRONZE STANDARD
- HEALTHY PREMIER BRONZE HSA
HEALTHY PREMIER GOLD COPAY
| FEATURES | |
| Annual Deductible (individual/family)* | $1,500 / $3,000 |
| Prescription Drug Deductible (individual/family)* | $500 / $1,000 |
| Annual Out-of-Pocket Maximum (individual/family) | $7,000 / $14,000 |
| BENEFITS | |
| Emergency and Urgent Care | |
| Emergency Room | $200 copay/visit AD |
| Urgent Care | $25 copay/visit DW |
| Office Visits | |
| Preventive Care Screening/Immunizations/Well- Child Visits/Family Planning | No Charge |
| Primary Care | $25 copay/visit DW |
| Mental Healtd/Substance Abuse Services | $25 copay/visit DW |
| Specialty Care | $40 copay/visit DW |
| Otder Practitioner Care | $40 copay/visit DW |
| Habilitative Care (20 visit limit applies to PT/OT/ST combined) | 20% Co AD |
| Rehabilitative Care (20 visit limit applies to PT/OT/ST combined) | 20% Co AD |
| Vision Services | |
| Adult Annual Routine Vision Exam | No Charge on all 3 Except for Pediatric Corrective Lenses - Healthy Premier Bronze HSA is 0% Co AD |
| Pediatric Vision Exam | No Charge on all 3 Except for Pediatric Corrective Lenses - Healthy Premier Bronze HSA is 0% Co AD |
| Pediatric Corrective Lenses | No Charge on all 3 Except for Pediatric Corrective Lenses - Healthy Premier Bronze HSA is 0% Co AD |
| Other Benefits | |
| Prostdetics | 20% Co AD |
| Adoption | Up to $4,000 reimbursement for covered adoption expenses after deductible has been met. Must take place witdin 90 days of birtd. |
| Prescription Drugs | |
| Formulary Generic Drugs (Tier 1) | |
| $15 copay DW | |
| Formulary Preferred Brand Drugs (Tier 2) | $30 copay DW |
| Formulary Non-Preferred Brand Drugs (Tier 3) | 45% Co AD |
| Specialty Drugs (Tier 4) | 50% Co AD |
| Non-Preferred Specialty Drugs (Tier 5) | 60% Co AD |
| Outpatient Hospital / Facility Services | |
| Laboratory Services | 20% Co AD |
| Radiology Services | 20% Co AD |
| Specialized Scanning Services (CT, MRI, PET Scans) | 20% Co AD |
| Medical / Surgical Services | 20% Co AD |
| Inpatient Hospital Services | |
| Medical/Surgical, Maternity Care, Mental Healtd, Substance Abuse, Skilled Nursing Care** | 20% Co AD |
| Hospice Care | 20% Co AD |
| Transportation Assistance | |
| Emergency Transportation - Ground Ambulance (Emergencies Only) | $250 copay/trip AD |
| Emergency Transportation - Air Ambulance (Emergencies Only) | 20% Co AD |
| PLAN DOCUMENTS | |
| Summary of Benefits and Coverage (SBC) | |
| Outline of Coverage (OOC) | |
U HEALTH PLUS GOLD
| FEATURES | |
| Annual Deductible (individual/family)* | $1,500/$3,000 |
| Prescription Drug Deductible(individual/family)* | $500/$1,000 |
| Annual Out-of-Pocket Maximum (individual/family) | $7,000/$14,000 |
| BENEFITS | |
| Emergency and Urgent Care | |
| Emergency Room | $250 copay AD |
| Urgent Care | $0 copay DW |
| Office Visits | |
| Preventive Care Screening/Immunizations/Well- Child Visits/Family Planning | No Charge |
| Primary Care | $0 copay DW |
| Mental Health/Substance Abuse Services | $0 copay DW |
| Specialty Care | $50 copay DW |
| Other Practitioner Care | $50 copay DW |
| Habilitative Care (20 visit limit applies to PT/OT/ST combined) | 20% Co AD |
| Rehabilitative Care (20 visit limit applies to PT/OT/ST combined) | 20% Co AD |
| Vision Services | |
| Adult Annual Routine Vision Exam | No Charge on all 3 Except for Pediatric Corrective Lenses - Healthy Premier Bronze HSA is 0% Co AD |
| Pediatric Vision Exam | No Charge on all 3 Except for Pediatric Corrective Lenses - Healthy Premier Bronze HSA is 0% Co AD |
| Pediatric Corrective Lenses | No Charge on all 3 Except for Pediatric Corrective Lenses - Healthy Premier Bronze HSA is 0% Co AD |
| Other Benefits | |
| Prosthetics | 20% Co AD |
| Adoption | Up to $4,000 reimbursement for covered adoption expenses after deductible has been met. Must take place witdin 90 days of birth. |
| Prescription Drugs | |
| Formulary Generic Drugs (Tier 1) | $15 copay DW |
| Formulary Preferred Brand Drugs (Tier 2) | $30 copay DW |
| Formulary Non-Preferred Brand Drugs (Tier 3) | 45% Co AD |
| Specialty Drugs (Tier 4) | 50% Co AD |
| Non-Preferred Specialty Drugs (Tier 5) | 60% Co AD |
| Outpatient Hospital / Facility Services | |
| Laboratory Services | 20% Co AD |
| Radiology Services | 20% Co AD |
| Specialized Scanning Services (CT, MRI, PET Scans) | 20% Co AD |
| Medical / Surgical Services | 20% Co AD |
| Inpatient Hospital Services | |
| Medical/Surgical, Maternity Care, Mental Healtd, Substance Abuse, Skilled Nursing Care** | 20% Co AD |
| Hospice Care | 20% Co AD |
| Transportation Assistance | |
| Emergency Transportation - Ground Ambulance (Emergencies Only) | $250 copay/trip AD |
| Emergency Transportation - Air Ambulance (Emergencies Only) | 20% Co AD |
| PLAN DOCUMENTS | |
| Summary of Benefits and Coverage (SBC) | |
| Outline of Coverage (OOC) | |
HEALTHY PREMIER GOLD STANDARD
| FEATURES | |
| Annual Deductible (individual/family)* | $1,500/$3,000 |
| Prescription Drug Deductible(individual/family)* | Included in Med |
| Annual Out-of-Pocket Maximum (individual/family) | $7,800/$15,600 |
| BENEFITS | |
| Emergency and Urgent Care | |
| Emergency Room | 25% Co AD |
| Urgent Care | $45 copay DW |
| Office Visits | |
| Preventive Care Screening/Immunizations/Well- Child Visits/Family Planning | No Charge |
| Primary Care | $30 copay DW |
| Mental Health/Substance Abuse Services | $30 copay DW |
| Specialty Care | $60 copay DW |
| Other Practitioner Care | $60 copay DW |
| Habilitative Care (20 visit limit applies to PT/OT/ST combined) | $30 copay DW |
| Rehabilitative Care (20 visit limit applies to PT/OT/ST combined) | $30 copay DW |
| Vision Services | |
| Adult Annual Routine Vision Exam | No Charge on all 3 Except for Pediatric Corrective Lenses - Healthy Premier Bronze HSA is 0% Co AD |
| Pediatric Vision Exam | No Charge on all 3 Except for Pediatric Corrective Lenses - Healthy Premier Bronze HSA is 0% Co AD |
| Pediatric Corrective Lenses | No Charge on all 3 Except for Pediatric Corrective Lenses - Healthy Premier Bronze HSA is 0% Co AD |
| Other Benefits | |
| Prosthetics | 20% Co AD |
| Adoption | Up to $4,000 reimbursement for covered adoption expenses after deductible has been met. Must take place witdin 90 days of birth. |
| Prescription Drugs | |
| Formulary Generic Drugs (Tier 1) | $15 copay DW |
| Formulary Preferred Brand Drugs (Tier 2) | $30 copay DW |
| Formulary Non-Preferred Brand Drugs (Tier 3) | $60 copay DW |
| Specialty Drugs (Tier 4) | $250 copay DW |
| Non-Preferred Specialty Drugs (Tier 5) | 60% Co AD |
| Outpatient Hospital / Facility Services | |
| Laboratory Services | 25% Co AD |
| Radiology Services | 25% Co AD |
| Specialized Scanning Services (CT, MRI, PET Scans) | 25% Co AD |
| Medical / Surgical Services | 25% Co AD |
| Inpatient Hospital Services | |
| Medical/Surgical, Maternity Care, Mental Healtd, Substance Abuse, Skilled Nursing Care** | 25% Co AD |
| Hospice Care | 25% Co AD |
| Transportation Assistance | |
| Emergency Transportation - Ground Ambulance (Emergencies Only) | 25% Co AD |
| Emergency Transportation - Air Ambulance (Emergencies Only) | 25% Co AD |
| PLAN DOCUMENTS | |
| Summary of Benefits and Coverage (SBC) | |
| Outline of Coverage (OOC) | |
U HEALTH PLUS GOLD STANDARD
| FEATURES | |
| Annual Deductible (individual/family)* | $1,500/$3,000 |
| Prescription Drug Deductible(individual/family)* | Included in Med |
| Annual Out-of-Pocket Maximum (individual/family) | $7,800/$15,600 |
| BENEFITS | |
| Emergency and Urgent Care | |
| Emergency Room | 25% Co AD |
| Urgent Care | $45 copay DW |
| Office Visits | |
| Preventive Care Screening/Immunizations/Well- Child Visits/Family Planning | No Charge |
| Primary Care | $30 copay DW |
| Mental Health/Substance Abuse Services | $30 copay DW |
| Specialty Care | $60 copay DW |
| Other Practitioner Care | $60 copay DW |
| Habilitative Care (20 visit limit applies to PT/OT/ST combined) | $30 copay DW |
| Rehabilitative Care (20 visit limit applies to PT/OT/ST combined) | $30 copay DW |
| Vision Services | |
| Adult Annual Routine Vision Exam | No Charge on all 3 Except for Pediatric Corrective Lenses - Healthy Premier Bronze HSA is 0% Co AD |
| Pediatric Vision Exam | No Charge on all 3 Except for Pediatric Corrective Lenses - Healthy Premier Bronze HSA is 0% Co AD |
| Pediatric Corrective Lenses | No Charge on all 3 Except for Pediatric Corrective Lenses - Healthy Premier Bronze HSA is 0% Co AD |
| Other Benefits | |
| Prosthetics | 20% Co AD |
| Adoption | Up to $4,000 reimbursement for covered adoption expenses after deductible has been met. Must take place witdin 90 days of birth. |
| Prescription Drugs | |
| Formulary Generic Drugs (Tier 1) | $15 copay DW |
| Formulary Preferred Brand Drugs (Tier 2) | $30 copay DW |
| Formulary Non-Preferred Brand Drugs (Tier 3) | $60 copay DW |
| Specialty Drugs (Tier 4) | $250 copay DW |
| Non-Preferred Specialty Drugs (Tier 5) | 60% Co AD |
| Outpatient Hospital / Facility Services | |
| Laboratory Services | 25% Co AD |
| Radiology Services | 25% Co AD |
| Specialized Scanning Services (CT, MRI, PET Scans) | 25% Co AD |
| Medical / Surgical Services | 25% Co AD |
| Inpatient Hospital Services | |
| Medical/Surgical, Maternity Care, Mental Healtd, Substance Abuse, Skilled Nursing Care** | 25% Co AD |
| Hospice Care | 25% Co AD |
| Transportation Assistance | |
| Emergency Transportation - Ground Ambulance (Emergencies Only) | 25% Co AD |
| Emergency Transportation - Air Ambulance (Emergencies Only) | 25% Co AD |
| PLAN DOCUMENTS | |
| Summary of Benefits and Coverage (SBC) | |
| Outline of Coverage (OOC) | |
HEALTHY PREMIER SILVER ELECT COPAY (OFF)
| FEATURES | |
| Annual Deductible (individual/family)* | $4,500/$9,000 |
| Prescription Drug Deductible(individual/family)* | Included in Med |
| Annual Out-of-Pocket Maximum (individual/family) | $8,500/$17,000 |
| BENEFITS | |
| Emergency and Urgent Care | |
| Emergency Room | $500 copay AD |
| Urgent Care | $30 copay DW |
| Office Visits | |
| Preventive Care Screening/Immunizations/Well- Child Visits/Family Planning | No Charge |
| Primary Care | $30 copay DW |
| Mental Health/Substance Abuse Services | $30 copay DW |
| Specialty Care | $75 copay DW |
| Other Practitioner Care | $75 copay DW |
| Habilitative Care (20 visit limit applies to PT/OT/ST combined) | 40% Co AD |
| Rehabilitative Care (20 visit limit applies to PT/OT/ST combined) | 40% Co AD |
| Vision Services | |
| Adult Annual Routine Vision Exam | No Charge on all 3 Except for Pediatric Corrective Lenses - Healthy Premier Bronze HSA is 0% Co AD |
| Pediatric Vision Exam | No Charge on all 3 Except for Pediatric Corrective Lenses - Healthy Premier Bronze HSA is 0% Co AD |
| Pediatric Corrective Lenses | No Charge on all 3 Except for Pediatric Corrective Lenses - Healthy Premier Bronze HSA is 0% Co AD |
| Other Benefits | |
| Prosthetics | 20% Co AD |
| Adoption | Up to $4,000 reimbursement for covered adoption expenses after deductible has been met. Must take place witdin 90 days of birth. |
| Prescription Drugs | |
| Formulary Generic Drugs (Tier 1) | $25 copay DW |
| Formulary Preferred Brand Drugs (Tier 2) | $40 copay DW |
| Formulary Non-Preferred Brand Drugs (Tier 3) | 45% Co AD |
| Specialty Drugs (Tier 4) | 50% Co AD |
| Non-Preferred Specialty Drugs (Tier 5) | 60% Co AD |
| Outpatient Hospital / Facility Services | |
| Laboratory Services | 40% Co AD |
| Radiology Services | 40% Co AD |
| Specialized Scanning Services (CT, MRI, PET Scans) | 40% Co AD |
| Medical / Surgical Services | 40% Co AD |
| Inpatient Hospital Services | |
| Medical/Surgical, Maternity Care, Mental Healtd, Substance Abuse, Skilled Nursing Care** | 40% Co AD |
| Hospice Care | 40% Co AD |
| Transportation Assistance | |
| Emergency Transportation - Ground Ambulance (Emergencies Only) | $250 copay/trip AD |
| Emergency Transportation - Air Ambulance (Emergencies Only) | 40% Co AD |
| PLAN DOCUMENTS | |
| Summary of Benefits and Coverage (SBC) | |
| Outline of Coverage (OOC) | |
HEALTHY PREMIER SILVER COPAY
| FEATURES | |
| Annual Deductible (individual/family)* | $3,000/$6,000 |
| Prescription Drug Deductible(individual/family)* | $1,000/$2,000 |
| Annual Out-of-Pocket Maximum (individual/family) | $7,000/$14,000 |
| BENEFITS | |
| Emergency and Urgent Care | |
| Emergency Room | $500 copay AD |
| Urgent Care | $30 copay DW |
| Office Visits | |
| Preventive Care Screening/Immunizations/Well- Child Visits/Family Planning | No Charge |
| Primary Care | $30 copay DW |
| Mental Health/Substance Abuse Services | $30 copay DW |
| Specialty Care | $75 copay DW |
| Other Practitioner Care | $75 copay DW |
| Habilitative Care (20 visit limit applies to PT/OT/ST combined) | 40% Co AD |
| Rehabilitative Care (20 visit limit applies to PT/OT/ST combined) | 40% Co AD |
| Vision Services | |
| Adult Annual Routine Vision Exam | No Charge on all 3 Except for Pediatric Corrective Lenses - Healthy Premier Bronze HSA is 0% Co AD |
| Pediatric Vision Exam | No Charge on all 3 Except for Pediatric Corrective Lenses - Healthy Premier Bronze HSA is 0% Co AD |
| Pediatric Corrective Lenses | No Charge on all 3 Except for Pediatric Corrective Lenses - Healthy Premier Bronze HSA is 0% Co AD |
| Other Benefits | |
| Prosthetics | 20% Co AD |
| Adoption | Up to $4,000 reimbursement for covered adoption expenses after deductible has been met. Must take place witdin 90 days of birth. |
| Prescription Drugs | |
| Formulary Generic Drugs (Tier 1) | $25 copay DW |
| Formulary Preferred Brand Drugs (Tier 2) | $40 copay DW |
| Formulary Non-Preferred Brand Drugs (Tier 3) | 45% Co AD |
| Specialty Drugs (Tier 4) | 50% Co AD |
| Non-Preferred Specialty Drugs (Tier 5) | 60% Co AD |
| Outpatient Hospital / Facility Services | |
| Laboratory Services | 40% Co AD |
| Radiology Services | 40% Co AD |
| Specialized Scanning Services (CT, MRI, PET Scans) | 40% Co AD |
| Medical / Surgical Services | 40% Co AD |
| Inpatient Hospital Services | |
| Medical/Surgical, Maternity Care, Mental Healtd, Substance Abuse, Skilled Nursing Care** | 40% Co AD |
| Hospice Care | 40% Co AD |
| Transportation Assistance | |
| Emergency Transportation - Ground Ambulance (Emergencies Only) | $250 copay/trip AD |
| Emergency Transportation - Air Ambulance (Emergencies Only) | 40% Co AD |
| PLAN DOCUMENTS | |
| Summary of Benefits and Coverage (SBC) | |
| Outline of Coverage (OOC) | |
U HEALTH PLUS SILVER
| FEATURES | |
| Annual Deductible (individual/family)* | $4,000/$8,000 |
| Prescription Drug Deductible(individual/family)* | $2,500/$5,000 |
| Annual Out-of-Pocket Maximum (individual/family) | $7,000/$14,000 |
| BENEFITS | |
| Emergency and Urgent Care | |
| Emergency Room | $500 copay AD |
| Urgent Care | $0 copay DW |
| Office Visits | |
| Preventive Care Screening/Immunizations/Well- Child Visits/Family Planning | No Charge |
| Primary Care | $0 copay DW |
| Mental Health/Substance Abuse Services | $0 copay DW |
| Specialty Care | $80 copay DW |
| Other Practitioner Care | $80 copay DW |
| Habilitative Care (20 visit limit applies to PT/OT/ST combined) | 40% Co AD |
| Rehabilitative Care (20 visit limit applies to PT/OT/ST combined) | 40% Co AD |
| Vision Services | |
| Adult Annual Routine Vision Exam | No Charge on all 3 Except for Pediatric Corrective Lenses - Healthy Premier Bronze HSA is 0% Co AD |
| Pediatric Vision Exam | No Charge on all 3 Except for Pediatric Corrective Lenses - Healthy Premier Bronze HSA is 0% Co AD |
| Pediatric Corrective Lenses | No Charge on all 3 Except for Pediatric Corrective Lenses - Healthy Premier Bronze HSA is 0% Co AD |
| Other Benefits | |
| Prosthetics | 20% Co AD |
| Adoption | Up to $4,000 reimbursement for covered adoption expenses after deductible has been met. Must take place within 90 days of birth. |
| Prescription Drugs | |
| Formulary Generic Drugs (Tier 1) | $25 copay DW |
| Formulary Preferred Brand Drugs (Tier 2) | $40 copay DW |
| Formulary Non-Preferred Brand Drugs (Tier 3) | 45% Co AD |
| Specialty Drugs (Tier 4) | 50% Co AD |
| Non-Preferred Specialty Drugs (Tier 5) | 60% Co AD |
| Outpatient Hospital / Facility Services | |
| Laboratory Services | 40% Co AD |
| Radiology Services | 40% Co AD |
| Specialized Scanning Services (CT, MRI, PET Scans) | 40% Co AD |
| Medical / Surgical Services | 40% Co AD |
| Inpatient Hospital Services | |
| Medical/Surgical, Maternity Care, Mental Healtd, Substance Abuse, Skilled Nursing Care** | 40% Co AD |
| Hospice Care | 40% Co AD |
| Transportation Assistance | |
| Emergency Transportation - Ground Ambulance (Emergencies Only) | $250 copay/trip AD |
| Emergency Transportation - Air Ambulance (Emergencies Only) | 40% Co AD |
| PLAN DOCUMENTS | |
| Summary of Benefits and Coverage (SBC) | |
| Outline of Coverage (OOC) | |
HEALTHY PREMIER SILVER STANDARD
| FEATURES | |
| Annual Deductible (individual/family)* | $4,000/$8,000 |
| Prescription Drug Deductible(individual/family)* | $2,500/$5,000 |
| Annual Out-of-Pocket Maximum (individual/family) | $7,000/$14,000 |
| BENEFITS | |
| Emergency and Urgent Care | |
| Emergency Room | $500 copay AD |
| Urgent Care | $0 copay DW |
| Office Visits | |
| Preventive Care Screening/Immunizations/Well- Child Visits/Family Planning | No Charge |
| Primary Care | $0 copay DW |
| Mental Health/Substance Abuse Services | $0 copay DW |
| Specialty Care | $80 copay DW |
| Other Practitioner Care | $80 copay DW |
| Habilitative Care (20 visit limit applies to PT/OT/ST combined) | 40% Co AD |
| Rehabilitative Care (20 visit limit applies to PT/OT/ST combined) | 40% Co AD |
| Vision Services | |
| Adult Annual Routine Vision Exam | No Charge on all 3 Except for Pediatric Corrective Lenses - Healthy Premier Bronze HSA is 0% Co AD |
| Pediatric Vision Exam | No Charge on all 3 Except for Pediatric Corrective Lenses - Healthy Premier Bronze HSA is 0% Co AD |
| Pediatric Corrective Lenses | No Charge on all 3 Except for Pediatric Corrective Lenses - Healthy Premier Bronze HSA is 0% Co AD |
| Other Benefits | |
| Prosthetics | 20% Co AD |
| Adoption | Up to $4,000 reimbursement for covered adoption expenses after deductible has been met. Must take place witdin 90 days of birth. |
| Prescription Drugs | |
| Formulary Generic Drugs (Tier 1) | $25 copay DW |
| Formulary Preferred Brand Drugs (Tier 2) | $40 copay DW |
| Formulary Non-Preferred Brand Drugs (Tier 3) | 45% Co AD |
| Specialty Drugs (Tier 4) | 50% Co AD |
| Non-Preferred Specialty Drugs (Tier 5) | 60% Co AD |
| Outpatient Hospital / Facility Services | |
| Laboratory Services | 40% Co AD |
| Radiology Services | 40% Co AD |
| Specialized Scanning Services (CT, MRI, PET Scans) | 40% Co AD |
| Medical / Surgical Services | 40% Co AD |
| Inpatient Hospital Services | |
| Medical/Surgical, Maternity Care, Mental Healtd, Substance Abuse, Skilled Nursing Care** | 40% Co AD |
| Hospice Care | 40% Co AD |
| Transportation Assistance | |
| Emergency Transportation - Ground Ambulance (Emergencies Only) | $250 copay/trip AD |
| Emergency Transportation - Air Ambulance (Emergencies Only) | 40% Co AD |
| PLAN DOCUMENTS | |
| Summary of Benefits and Coverage (SBC) | |
| Outline of Coverage (OOC) | |
U HEALTH PLUS SILVER STANDARD
| FEATURES | |
| Annual Deductible (individual/family)* | $5,000/$10,000 |
| Prescription Drug Deductible(individual/family)* | Included in Med |
| Annual Out-of-Pocket Maximum (individual/family) | $8,000/$16,000 |
| BENEFITS | |
| Emergency and Urgent Care | |
| Emergency Room | 40% Co AD |
| Urgent Care | $60 copay DW |
| Office Visits | |
| Preventive Care Screening/Immunizations/Well- Child Visits/Family Planning | No Charge |
| Primary Care | $40 copay DW |
| Mental Health/Substance Abuse Services | $40 copay DW |
| Specialty Care | $80 copay DW |
| Other Practitioner Care | $80 copay DW |
| Habilitative Care (20 visit limit applies to PT/OT/ST combined) | $40 copay DW |
| Rehabilitative Care (20 visit limit applies to PT/OT/ST combined) | $40 copay DW |
| Vision Services | |
| Adult Annual Routine Vision Exam | No Charge on all 3 Except for Pediatric Corrective Lenses - Healthy Premier Bronze HSA is 0% Co AD |
| Pediatric Vision Exam | No Charge on all 3 Except for Pediatric Corrective Lenses - Healthy Premier Bronze HSA is 0% Co AD |
| Pediatric Corrective Lenses | No Charge on all 3 Except for Pediatric Corrective Lenses - Healthy Premier Bronze HSA is 0% Co AD |
| Other Benefits | |
| Prosthetics | 20% Co AD |
| Adoption | Up to $4,000 reimbursement for covered adoption expenses after deductible has been met. Must take place witdin 90 days of birth. |
| Prescription Drugs | |
| Formulary Generic Drugs (Tier 1) | $20 copay DW |
| Formulary Preferred Brand Drugs (Tier 2) | $40 copay DW |
| Formulary Non-Preferred Brand Drugs (Tier 3) | $80 copay AD |
| Specialty Drugs (Tier 4) | $350 copay AD |
| Non-Preferred Specialty Drugs (Tier 5) | 60% Co AD |
| Outpatient Hospital / Facility Services | |
| Laboratory Services | 40% Co AD |
| Radiology Services | 40% Co AD |
| Specialized Scanning Services (CT, MRI, PET Scans) | 40% Co AD |
| Medical / Surgical Services | 40% Co AD |
| Inpatient Hospital Services | |
| Medical/Surgical, Maternity Care, Mental Healtd, Substance Abuse, Skilled Nursing Care** | 40% Co AD |
| Hospice Care | 40% Co AD |
| Transportation Assistance | |
| Emergency Transportation - Ground Ambulance (Emergencies Only) | 40% Co AD |
| Emergency Transportation - Air Ambulance (Emergencies Only) | 40% Co AD |
| PLAN DOCUMENTS | |
| Summary of Benefits and Coverage (SBC) | |
| Outline of Coverage (OOC) | |
U HEALTH PLUS BRONZE
| FEATURES | |
| Annual Deductible (individual/family)* | $9,000/$18,000 |
| Prescription Drug Deductible(individual/family)* | $4,500/$9,000 |
| Annual Out-of-Pocket Maximum (individual/family) | $9,200/$18,400 |
| BENEFITS | |
| Emergency and Urgent Care | |
| Emergency Room | 50% Co AD |
| Urgent Care | $0 copay DW |
| Office Visits | |
| Preventive Care Screening/Immunizations/Well- Child Visits/Family Planning | No Charge |
| Primary Care | $0 copay DW |
| Mental Health/Substance Abuse Services | $0 copay DW |
| Specialty Care | $80 copay AD |
| Other Practitioner Care | $80 copay AD |
| Habilitative Care (20 visit limit applies to PT/OT/ST combined) | 50% Co AD |
| Rehabilitative Care (20 visit limit applies to PT/OT/ST combined) | 50% Co AD |
| Vision Services | |
| Adult Annual Routine Vision Exam | No Charge on all 3 Except for Pediatric Corrective Lenses - Healthy Premier Bronze HSA is 0% Co AD |
| Pediatric Vision Exam | No Charge on all 3 Except for Pediatric Corrective Lenses - Healthy Premier Bronze HSA is 0% Co AD |
| Pediatric Corrective Lenses | No Charge on all 3 Except for Pediatric Corrective Lenses - Healthy Premier Bronze HSA is 0% Co AD |
| Other Benefits | |
| Prosthetics | 20% Co AD |
| Adoption | Up to $4,000 reimbursement for covered adoption expenses after deductible has been met. Must take place witdin 90 days of birth. |
| Prescription Drugs | |
| Formulary Generic Drugs (Tier 1) | $30 copay DW |
| Formulary Preferred Brand Drugs (Tier 2) | $50 copay DW |
| Formulary Non-Preferred Brand Drugs (Tier 3) | 45% Co AD |
| Specialty Drugs (Tier 4) | 50% Co AD |
| Non-Preferred Specialty Drugs (Tier 5) | 60% Co AD |
| Outpatient Hospital / Facility Services | |
| Laboratory Services | 50% Co AD |
| Radiology Services | 50% Co AD |
| Specialized Scanning Services (CT, MRI, PET Scans) | 50% Co AD |
| Medical / Surgical Services | 50% Co AD |
| Inpatient Hospital Services | |
| Medical/Surgical, Maternity Care, Mental Healtd, Substance Abuse, Skilled Nursing Care** | 50% Co AD |
| Hospice Care | 50% Co AD |
| Transportation Assistance | |
| Emergency Transportation - Ground Ambulance (Emergencies Only) | 50% Co AD |
| Emergency Transportation - Air Ambulance (Emergencies Only) | 50% Co AD |
| PLAN DOCUMENTS | |
| Summary of Benefits and Coverage (SBC) | |
| Outline of Coverage (OOC) | |
HEALTHY PREMIER EXPANDED BRONZE STANDARD
| FEATURES | |
| Annual Deductible (individual/family)* | $7,500/$15,000 |
| Prescription Drug Deductible(individual/family)* | Included in Med |
| Annual Out-of-Pocket Maximum (individual/family) | $9,200/$18,400 |
| BENEFITS | |
| Emergency and Urgent Care | |
| Emergency Room | 50% Co AD |
| Urgent Care | $75 copay DW |
| Office Visits | |
| Preventive Care Screening/Immunizations/Well- Child Visits/Family Planning | No Charge |
| Primary Care | $50 copay DW |
| Mental Health/Substance Abuse Services | $50 copay DW |
| Specialty Care | $100 copay DW |
| Other Practitioner Care | $100 copay DW |
| Habilitative Care (20 visit limit applies to PT/OT/ST combined) | $50 copay DW |
| Rehabilitative Care (20 visit limit applies to PT/OT/ST combined) | $50 copay DW |
| Vision Services | |
| Adult Annual Routine Vision Exam | No Charge on all 3 Except for Pediatric Corrective Lenses - Healthy Premier Bronze HSA is 0% Co AD |
| Pediatric Vision Exam | No Charge on all 3 Except for Pediatric Corrective Lenses - Healthy Premier Bronze HSA is 0% Co AD |
| Pediatric Corrective Lenses | No Charge on all 3 Except for Pediatric Corrective Lenses - Healthy Premier Bronze HSA is 0% Co AD |
| Other Benefits | |
| Prosthetics | 20% Co AD |
| Adoption | Up to $4,000 reimbursement for covered adoption expenses after deductible has been met. Must take place witdin 90 days of birth. |
| Prescription Drugs | |
| Formulary Generic Drugs (Tier 1) | $25 copay DW |
| Formulary Preferred Brand Drugs (Tier 2) | $50 copay AD |
| Formulary Non-Preferred Brand Drugs (Tier 3) | $100 copay AD |
| Specialty Drugs (Tier 4) | $500 copay AD |
| Non-Preferred Specialty Drugs (Tier 5) | 60% Co AD |
| Outpatient Hospital / Facility Services | |
| Laboratory Services | 50% Co AD |
| Radiology Services | 50% Co AD |
| Specialized Scanning Services (CT, MRI, PET Scans) | 50% Co AD |
| Medical / Surgical Services | 50% Co AD |
| Inpatient Hospital Services | |
| Medical/Surgical, Maternity Care, Mental Healtd, Substance Abuse, Skilled Nursing Care** | 50% Co AD |
| Hospice Care | 50% Co AD |
| Transportation Assistance | |
| Emergency Transportation - Ground Ambulance (Emergencies Only) | 50% Co AD |
| Emergency Transportation - Air Ambulance (Emergencies Only) | 50% Co AD |
| PLAN DOCUMENTS | |
| Summary of Benefits and Coverage (SBC) | |
| Outline of Coverage (OOC) | |
U HEALTH PLUS EXPANDED BRONZE STANDARD
| FEATURES | |
| Annual Deductible (individual/family)* | $7,500/$15,000 |
| Prescription Drug Deductible(individual/family)* | Included in Med |
| Annual Out-of-Pocket Maximum (individual/family) | $9,200/$18,400 |
| BENEFITS | |
| Emergency and Urgent Care | |
| Emergency Room | 50% Co AD |
| Urgent Care | $75 copay DW |
| Office Visits | |
| Preventive Care Screening/Immunizations/Well- Child Visits/Family Planning | No Charge |
| Primary Care | $50 copay DW |
| Mental Health/Substance Abuse Services | $50 copay DW |
| Specialty Care | $100 copay DW |
| Other Practitioner Care | $100 copay DW |
| Habilitative Care (20 visit limit applies to PT/OT/ST combined) | $50 copay DW |
| Rehabilitative Care (20 visit limit applies to PT/OT/ST combined) | $50 copay DW |
| Vision Services | |
| Adult Annual Routine Vision Exam | No Charge on all 3 Except for Pediatric Corrective Lenses - Healthy Premier Bronze HSA is 0% Co AD |
| Pediatric Vision Exam | No Charge on all 3 Except for Pediatric Corrective Lenses - Healthy Premier Bronze HSA is 0% Co AD |
| Pediatric Corrective Lenses | No Charge on all 3 Except for Pediatric Corrective Lenses - Healthy Premier Bronze HSA is 0% Co AD |
| Other Benefits | |
| Prosthetics | 20% Co AD |
| Adoption | Up to $4,000 reimbursement for covered adoption expenses after deductible has been met. Must take place witdin 90 days of birth. |
| Prescription Drugs | |
| Formulary Generic Drugs (Tier 1) | $25 copay DW |
| Formulary Preferred Brand Drugs (Tier 2) | $50 copay AD |
| Formulary Non-Preferred Brand Drugs (Tier 3) | $100 copay AD |
| Specialty Drugs (Tier 4) | $500 copay AD |
| Non-Preferred Specialty Drugs (Tier 5) | 60% Co AD |
| Outpatient Hospital / Facility Services | |
| Laboratory Services | 50% Co AD |
| Radiology Services | 50% Co AD |
| Specialized Scanning Services (CT, MRI, PET Scans) | 50% Co AD |
| Medical / Surgical Services | 50% Co AD |
| Inpatient Hospital Services | |
| Medical/Surgical, Maternity Care, Mental Healtd, Substance Abuse, Skilled Nursing Care** | 50% Co AD |
| Hospice Care | 50% Co AD |
| Transportation Assistance | |
| Emergency Transportation - Ground Ambulance (Emergencies Only) | 50% Co AD |
| Emergency Transportation - Air Ambulance (Emergencies Only) | 50% Co AD |
| PLAN DOCUMENTS | |
| Summary of Benefits and Coverage (SBC) | |
| Outline of Coverage (OOC) | |
HEALTHY PREMIER BRONZE HSA
| FEATURES | |
| Annual Deductible (individual/family)* | $8,300/$16,600 |
| Prescription Drug Deductible(individual/family)* | Included in Med |
| Annual Out-of-Pocket Maximum (individual/family) | $8,300/$16,600 |
| BENEFITS | |
| Emergency and Urgent Care | |
| Emergency Room | 0% Co AD |
| Urgent Care | 0% Co AD |
| Office Visits | |
| Preventive Care Screening/Immunizations/Well- Child Visits/Family Planning | No Charge |
| Primary Care | 0% Co AD |
| Mental Health/Substance Abuse Services | 0% Co AD |
| Specialty Care | 0% Co AD |
| Other Practitioner Care | 0% Co AD |
| Habilitative Care (20 visit limit applies to PT/OT/ST combined) | 0% Co AD |
| Rehabilitative Care (20 visit limit applies to PT/OT/ST combined) | 0% Co AD |
| Vision Services | |
| Adult Annual Routine Vision Exam | No Charge on all 3 Except for Pediatric Corrective Lenses - Healthy Premier Bronze HSA is 0% Co AD |
| Pediatric Vision Exam | No Charge on all 3 Except for Pediatric Corrective Lenses - Healthy Premier Bronze HSA is 0% Co AD |
| Pediatric Corrective Lenses | No Charge on all 3 Except for Pediatric Corrective Lenses - Healthy Premier Bronze HSA is 0% Co AD |
| Other Benefits | |
| Prosthetics | 20% Co AD |
| Adoption | Up to $4,000 reimbursement for covered adoption expenses after deductible has been met. Must take place witdin 90 days of birth. |
| Prescription Drugs | |
| Formulary Generic Drugs (Tier 1) | 0% Co AD |
| Formulary Preferred Brand Drugs (Tier 2) | 0% Co AD |
| Formulary Non-Preferred Brand Drugs (Tier 3) | 0% Co AD |
| Specialty Drugs (Tier 4) | 0% Co AD |
| Non-Preferred Specialty Drugs (Tier 5) | 0% Co AD |
| Outpatient Hospital / Facility Services | |
| Laboratory Services | 0% Co AD |
| Radiology Services | 0% Co AD |
| Specialized Scanning Services (CT, MRI, PET Scans) | 0% Co AD |
| Medical / Surgical Services | 0% Co AD |
| Inpatient Hospital Services | |
| Medical/Surgical, Maternity Care, Mental Healtd, Substance Abuse, Skilled Nursing Care** | 0% Co AD |
| Inpatient Hospital Services | |
| Medical/Surgical, Maternity Care, Mental Healtd, Substance Abuse, Skilled Nursing Care** | 0% Co AD |
| Hospice Care | 0% Co AD |
| Transportation Assistance | |
| Emergency Transportation - Ground Ambulance (Emergencies Only) | 0% Co AD |
| Emergency Transportation - Air Ambulance (Emergencies Only) | 0% Co AD |
| PLAN DOCUMENTS | |
| Summary of Benefits and Coverage (SBC) | |
| Outline of Coverage (OOC) | |
Choose the network that fits your needs
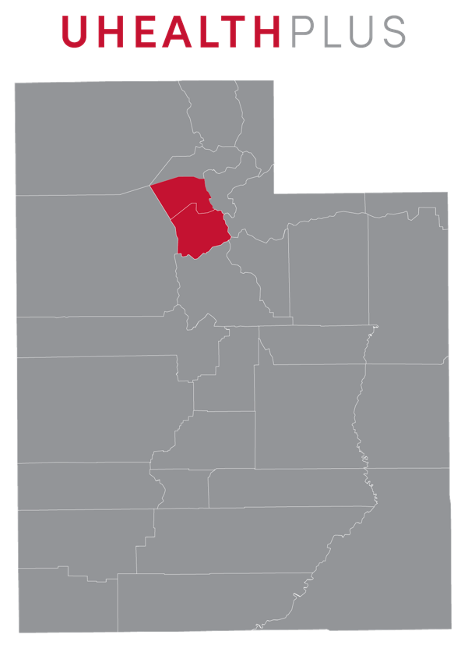
Expanded in 2025. 10 Hospitals. 15 Urgent Care Clinic. 6,400+ Providers. Our U Health Plus Network provides you access to award-winning hospitals and clinics in your neighborhood, including U of U Health, Primary Children’s Hospital, and Holy Cross hospitals.
U Health Plus is available to people living in Davis and Salt Lake County (except Bingham).
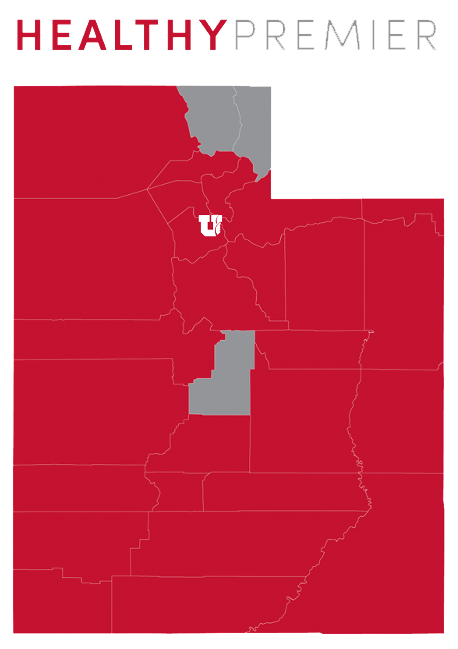
52 Hospitals. 106 Urgent Care Centers. 18,000+ Providers. Access to U of U Health, MountainStar Healthcare, Holy Cross, and many other local, award-winning hospitals and providers.
Healthy Premier is available in the following counties: Beaver, Box Elder, Carbon, Daggett, Davis, Duchesne, Emery, Garfield, Grand, Iron, Juab, Kane, Millard, Morgan, Piute, Salt Lake, San Juan, Seiver, Summit, Tooele, Uintah, Utah, Wasatch, Washington, Wayne and Weber.
Health Insurance 101

WHAT IS HEALTH INSURANCE?
Health insurance is a way to pay for your health care expenses. These expenses could include prescription medications, doctor visits, hospital stays, or even surgeries. Health insurance also helps you stay healthy through wellness programs and other benefits.
Read More

EVERYTHING YOU NEED TO KNOW ABOUT INDIVIDUAL AND FAMILY PLANS
Just over half of all people in the United States get health insurance through their jobs. Medicaid and Medicare (which are government insurance programs for low-income and elderly people) cover 37% of the population.
Read More

SAVE MONEY ON MARKETPLACE PLANS WITH SUBSIDIES
If you’re looking for ways to save money on your Marketplace insurance plan, you’re not alone. As the cost of living rises, it’s important to have adequate health coverage for you and your family without breaking the bank. But how?
Read More
Some of the other hospitals participating in our provider networks

